New Cancer Immunotherapy Combines Treatments, Explores Vaccines for Prevention
Serge Bulaev
Cancer immunotherapy is moving toward using combined treatments and exploring vaccines for people at higher risk. Studies suggest that pairing immunotherapies or adding them to other treatments may lead to longer remissions for some cancers. Early trials of vaccines to prevent cancer in certain high-risk groups, like those with genetic risks, show promise but still need more evidence. Experts note that matching treatments to each person's risk and timing may help, but some challenges like cost and complex regulations remain. There is still uncertainty about how long these benefits last and which patients will benefit most.
The future of cancer immunotherapy lies in combining treatments for durable control and developing preventive vaccines for high-risk individuals. This strategic shift moves beyond single therapies, focusing on coordinated tactics that yield deeper, longer-lasting remissions. The core principle is activating the immune system at the most opportune time - either when a tumor is most vulnerable or before it can form.
Combination strategies aim for longer remissions
By pairing different immunotherapies or adding them to treatments like chemotherapy, doctors can attack cancer from multiple angles. This approach overcomes tumor resistance and creates a more robust, lasting immune response, leading to deeper and more durable remissions than single-agent therapies alone.
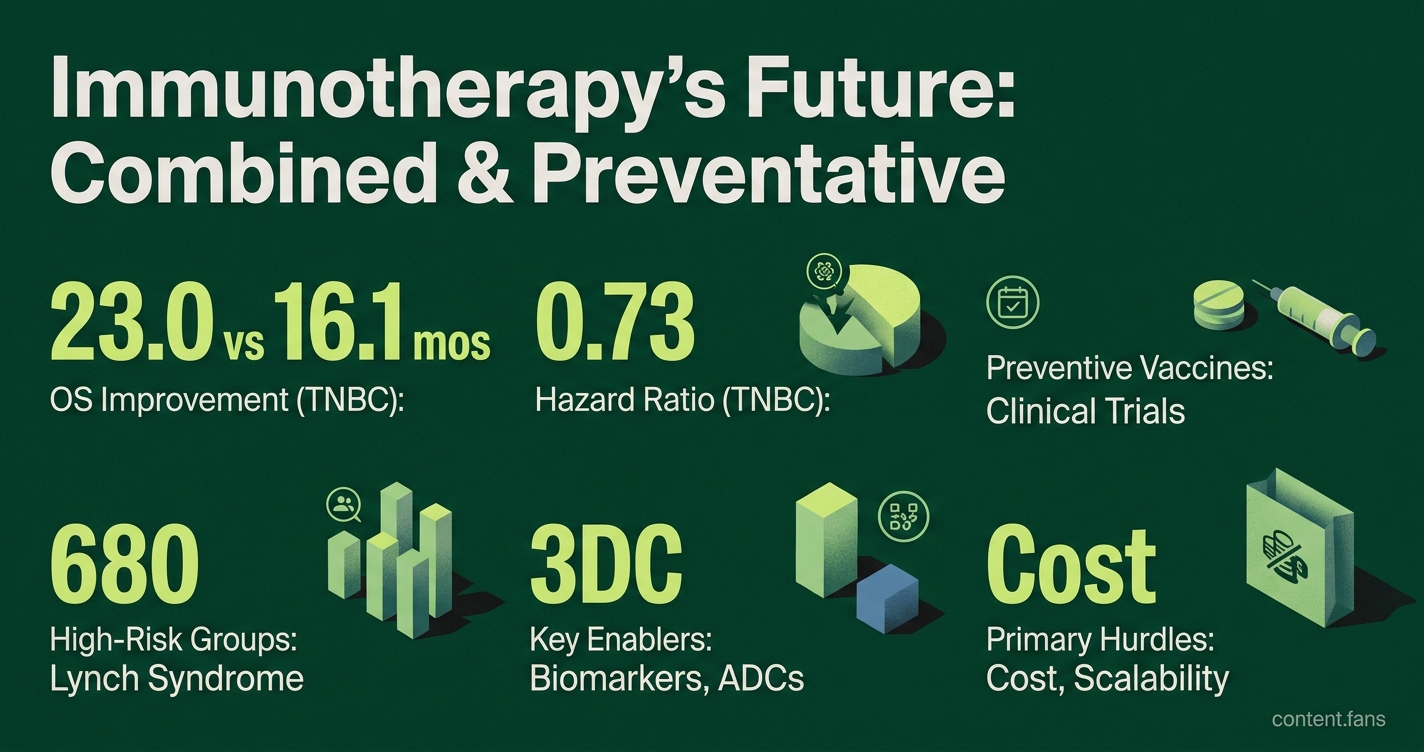
While checkpoint inhibitors are foundational, their effectiveness often plateaus when used alone. A peer-reviewed overview highlights combination immunotherapy as a key strategy to surpass these limits (Advances in cancer immunotherapy). In PD-L1 CPS ≥10 metastatic triple-negative breast cancer, pembrolizumab plus chemotherapy improved overall survival versus chemotherapy alone; the hazard ratio was about 0.73 and median OS was 23.0 vs 16.1 months. Furthermore, using circulating tumor DNA to guide post-surgery immunotherapy shows promise in converting temporary benefits into lasting remissions.
Vaccines explore interception in high risk groups
For non-viral cancers, preventive vaccines are still largely experimental but are making significant progress in clinical trials. Research is focused on "cancer interception" in high-risk populations. For example, according to industry reports, trials for individuals with Lynch syndrome have shown that experimental vaccines can spur immune responses and may reduce the formation of precancerous polyps (MD Anderson release). While current data primarily confirm safety and immune response, proving a reduction in cancer incidence requires larger trials. Nonetheless, institutional support is growing as the National Cancer Institute seeks immunoprevention agents for these groups.
Enablers and hurdles
Several key factors are advancing the field, while significant challenges remain.
- Enablers: Composite biomarkers, antibody-drug conjugates (ADCs), and advanced cell therapies are enabling more personalized and effective treatments. Real-time monitoring of circulating DNA helps optimize therapy and detect relapse early.
- Hurdles: The primary obstacles are regulatory complexity for novel agents, the scalability of manufacturing for personalized treatments, and prohibitive costs.
Key questions about the long-term durability of immunity and the true value of certain combinations versus their toxicity still need answers from ongoing late-stage trials. The current momentum is focused on creating rational treatment pairings that deepen immune response and developing targeted vaccines that could make some cancers preventable.
How are doctors combining different types of immunotherapy to achieve durable cures?
Several combinations are leading current clinical development, each designed to turn a short-term response into long-term remission.
-
Checkpoint blockade pairs - The dual PD-1 (pembrolizumab) + CTLA-4 (ipilimumab) regimen is now standard in metastatic melanoma and is being expanded to other tumor types. Clinical studies suggest this pairing may show enhanced tumor clearance and survival compared with single-agent therapy.
-
Immunotherapy + chemotherapy or ADCs - In triple-negative breast cancer, pembrolizumab plus chemotherapy improved overall survival in PD-L1 CPS ≥10 metastatic TNBC; the trial reported HR about 0.73 and median OS 23.0 vs 16.1 months. ADCs such as sacituzumab govitecan are being layered on top to further prolong benefit.
-
Post-surgery treatment guided by ctDNA - Memorial Sloan Kettering pilots show that a simple blood test can pick the patients most likely to benefit from adjuvant immunotherapy; a significant portion of patients cleared ctDNA after therapy and remained recurrence-free at follow-up.
-
Personalized mRNA vaccines added after ICI - An MSK pancreatic-cancer program reports that the autogene cevumeran vaccine kept tumor-specific T cells alive for extended periods in some recipients.
-
Cell therapy cocktails for "cold" tumors - Industry reports outline next-generation TIL, CAR-T and TCR therapies armed with microenvironment modifiers that can work in tumors previously unreachable by the immune system.
Put together, these combinations aim to prime the immune system, reduce tumor burden, and then lock in memory - a three-step recipe experts now see as the best shot at durable cures.
Which high-risk groups will soon be offered preventive cancer vaccines?
Several populations are moving to the front of clinical development.
-
Lynch syndrome - A Phase Ib/II trial of the NOUS-209 vaccine showed that immune targeting reduced precancerous lesions according to preliminary reports.
-
BRCA mutation carriers - University of Pennsylvania investigators are enrolling healthy BRCA-mutation individuals in a DNA-vaccine study designed to prevent breast cancer before it starts.
-
DCIS or premalignant breast lesions - A MUC1 vaccine is in Phase I testing for post-menopausal women with hormone-receptor-positive DCIS; the hope is to stop progression to invasive disease.
-
Rising CA-125 in ovarian-cancer survivors - A Cancer Vaccine Institute Phase II trial is giving a vaccine to patients whose blood tumor marker is climbing but who have no visible relapse on imaging, a classic interception scenario.
Outside of trials, today's only approved preventive cancer vaccines remain HPV and hepatitis B; every other candidate is still in early clinical stages, so participation in research studies is the only current path for most patients.
How are AI and biomarkers helping doctors choose the right immunotherapy before cancer even appears?
Composite, AI-driven blood signatures are beginning to guide clinical decisions.
-
Multimodal AI models now knit together genomics, proteomics, radiomics and clinical history into single response-risk scores. Research suggests these models may speed up biomarker discovery and anchor individualized treatment plans.
-
Blood-instead-of-biopsy - High-throughput plasma assays give a systems-level immune snapshot from a single tube of blood, allowing repeat testing without repeat biopsies.
-
Pre-therapy toxicity forecasts - A composite host-response model called PROphetirAE™ is being trained to flag patients at high risk of severe immune-related adverse events before the first infusion - a first in the field.
Preliminary data from BostonGene's platform show that baseline blood signatures can outperform traditional PD-L1 staining in predicting pembrolizumab response, but all tools remain under prospective validation.
What technical hurdles must still be solved for vaccine prevention to scale?
Manufacturing, regulation and cost are the big three barriers.
-
Manufacturing scalability - Personalized neoantigen vaccines are currently produced in small GMP lots for each patient. Moving to off-the-shelf libraries that still retain custom specificity is a key engineering focus.
-
Regulatory pathways - No vaccine for non-viral cancer has ever gained FDA approval as a preventive agent. Regulators must decide what endpoints are sufficient, since waiting decades for incidence reduction is impractical.
-
Cost and reimbursement - Projected price tags for a full neoantigen vaccine course exceed $200 000, far above the public-health threshold for a preventive agent. Consortium pricing and AI-driven epitope selection are being explored to drop costs.
Until these hurdles are crossed, preventive vaccination will remain a research-intensive luxury rather than standard care.
When will immunotherapy shift from treating existing cancer to preventing it altogether?
The shift has already started in clinical trials, but full population access is years away.
-
Current trials - Many new interception studies are enrolling, spanning breast, colon, pancreas, lung and Lynch-associated cancers.
-
Future inflection point - If ongoing trials demonstrate significant reductions in recurrence or high molecular response rates, regulators are expected to consider accelerated approval pathways for high-risk groups.
-
Early-adopter clinics - Academic centers like MSK, MD Anderson and Dana-Farber are already offering protocol-based vaccine access to BRCA or Lynch carriers who meet trial criteria.
Bottom line: the transition is underway, but the broad public-health pivot will depend on robust Phase III data and cost containment, a timeline many experts expect in the coming decade.